2 Jun 2021
An eye-opening set of blood and urine findings in a dog
Francesco Cian delves into another Diagnostic Dilemmas, this time for the case of a two-year-old neutered, female Yorkshire terrier with a history of weaness and lethargy.
Francesco Cian
Job Title
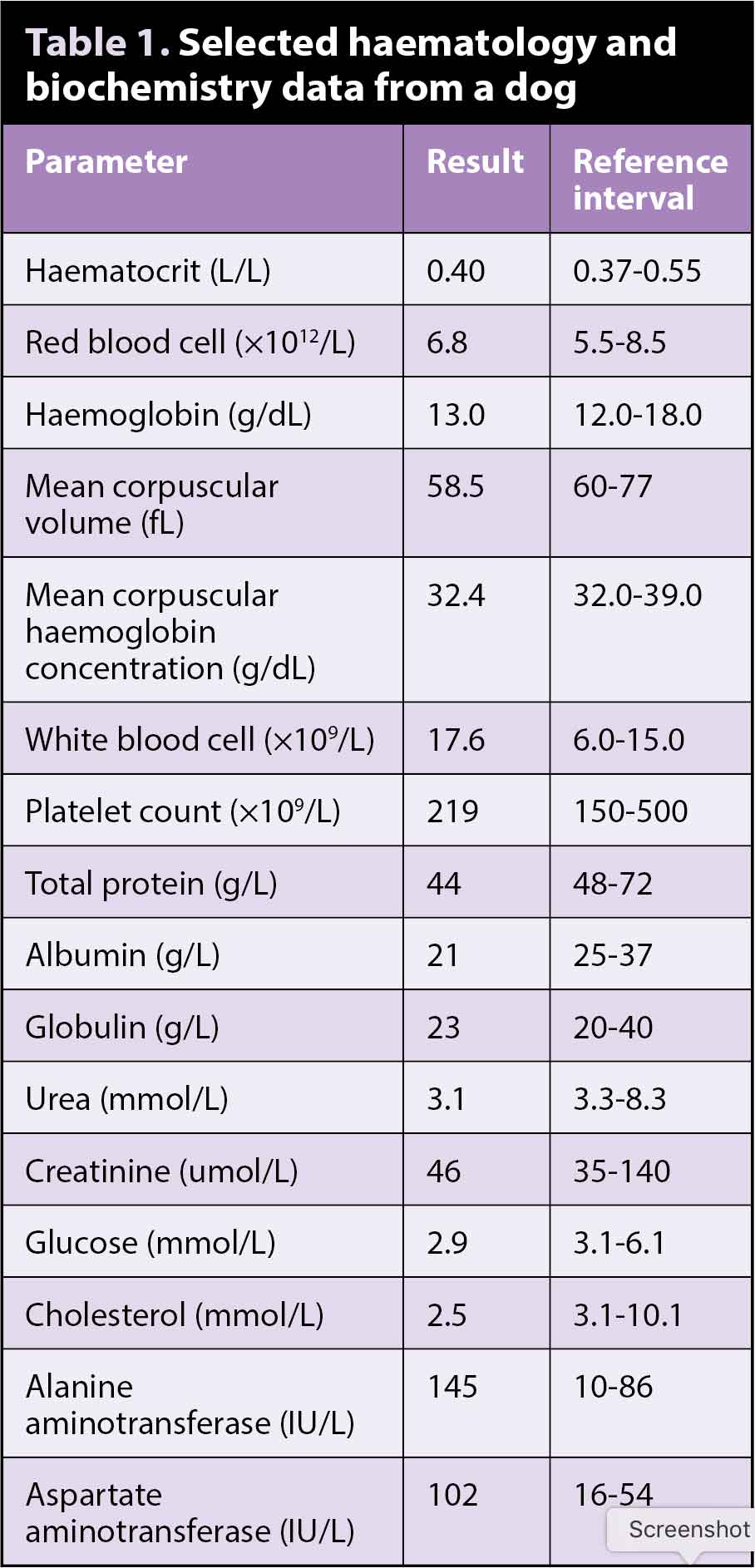
The laboratory data (Table 1) and the image (Figure 1) are from a two-year-old, neutered, female Yorkshire terrier with a few months’ history of weakness and lethargy. More recently, the dog had some episodes of vomiting, and experienced polyuria and polydipsia. No abnormalities were noted on physical examination.

The biochemistry findings showed a decrease in albumin, glucose, urea and cholesterol, and a mild elevation of liver enzymes.
Each of these changes may be due to several causes, ranging from pathological conditions (for example, hypoalbuminaemia secondary to intestinal or renal loss or inflammation) to spurious changes (for example, artifactual hypoglycaemia due to delayed sample examination). However, when genuine and present all together, these are considered highly suggestive for decreased hepatic function, since the liver is the organ where these substances are synthesised.
The veterinarian also performed a bile acid stimulation test that provided high results (91umol/L; reference range less than 10umol/L) and confirmed the initial suspicion.
Interestingly, the dog was not anaemic, but erythrocytes were microcytic (low mean corpuscular volume) and borderline hypochromic (low/normal mean corpuscular haemoglobin concentration), as often seen in patients with portosystemic shunt (PSS) – a condition commonly leading to liver dysfunction and often observed in young dogs.
PSS was further confirmed by the presence of ammonium urate crystals in urine and by imaging studies. Ammonium urate crystals (brown arrows) presented as round yellow-brownish structures with characteristic protrusions (“thorn apple” forms) and were admixed with few struvite crystals (red arrows).
Diagnosis
A diagnosis of PSS was given.
Follow-up
The dog underwent surgery. A single extrahepatic portocaval shunt was identified and an ameroid constrictor was placed.
Biopsy specimens collected at surgery were compatible with the presence of a shunt and were accompanied by mild periportal inflammation, which could have contributed to the raised liver enzymes and mild peripheral neutrophilia. A few weeks after surgery, the dog was reported as doing well at home.
Insight
PSS is an abnormal connection between the portal vascular system and systemic circulation. Blood from the abdominal organs, which should be drained by the portal vein into the liver, is instead shunted directly into the systemic circulation, bypassing the liver.
Shunts are often congenital due to abnormalities in the development of the portal venous system or fetal vessels. However, they may also be acquired as a result of portal hypertension caused by other liver disorders (for example, hepatic cirrhosis).
PSS may be extrahepatic (more common in small-breed dogs and cats) or intrahepatic (more often observed in large-breed dogs). Clinical signs vary and are not specific (for example, failure to thrive, chronic vomiting/diarrhoea, polyuria/polydipsia, poor recovery from anaesthesia). These are often episodic and may be more noticeable after eating.
A clinical syndrome known as hepatic encephalopathy and characterised by altered CNS function may occur as a failure of normal liver function and compromised hepatic ammonia detoxification.
The most common laboratory findings suggesting PSS include:
- reduced urea, albumin, glucose and/or cholesterol levels as a result of reduced functional liver mass
- increased serum bile acids and ammonia due to reduced clearance by the liver
- microcytosis (small red blood cells) with or without evidence of anaemia
The cause of these red blood cell changes is not fully understood, but has been attributed to a functional iron deficiency due to abnormal iron metabolism.
Urinalysis may reveal poorly concentrated urine, as a result of decreased production of urea by a dysfunctional liver and consequent reduction in the medullary hypertonicity affecting the ability of the kidneys to concentrate urine.
On sediment analysis, it is also common to observe the presence of characteristic ammonium biurate crystals, as a result of decreased metabolism and subsequent high serum concentrations of ammonia. These crystals can also be seen in certain canine breeds (for example, Dalmatians and bulldogs) in the absence of liver disease, and are due to an inherited defect in urate metabolism.
Take-home message
PSS may lack in typical clinical signs, but can often be identified by laboratory tests. These include evidence of liver dysfunction (low albumin, cholesterol glucose, urea, raised bile acids and ammonia), red blood cell microcytosis with/without anaemia, poorly concentrated urine and presence of characteristic ammonium biurate crystals on sediment analysis.